Vitamin B1
Vitamin B1 is a watersoluble vitamin. It consists out of a pyrimidine- and a thiazol ring, which are synthesized independently and linked afterwards.
Vitamin B1 is de novo produced by many plants and microorganisms. Humans and animals have to take it up by nutrition. They are only able to do the phosphorylation reaction of the thiamin molecule. Thiamin is found free and as mono-, di- and triphosphate. The different forms can be transfered into each other. The metabolic active form is thiamin diphosphate in the body and thiamin triphosphate in the brain.
Thiamin diphosphate (TDP) works as thermostable coenzyme in many enzymes of the carbohydrate and amino acid metabolism. In most reactions TDP catalyzes the cleavage of C-C bonds. In the nervous system vitamin B1 is needed for the stimulation of nerve cells.
The classical disease of patients with a lack of vitamin B1 is Beriberi, which is known from regions where people eating predominantly white rice. The symtoms are paralysis, muscle dystrophia and heart failure. Other diseases are the Wernicke encephalopathy, the Korsakow syndrome and some forms of the Landry`s paralysis. In industrialized countries alcoholism seems to be the most important reason for a lack of vitamin B1. In alcoholics the thiamin resorption is disturbed. Due to a damage of the liver the storage capacity of vitamin B1 is reduced.
Technical data
Sample EDTA-blood
Sample volume 50 µl
Detector Fluorescence Ex. 365 nm Em. 440 nm
Method isocratic
Determinations 100
Ordering Information
IC2201 Testkit
IC2201ko Controls (2 level each 250 µl lyoph.)
IC2201rp HPLC column
Principle of the method
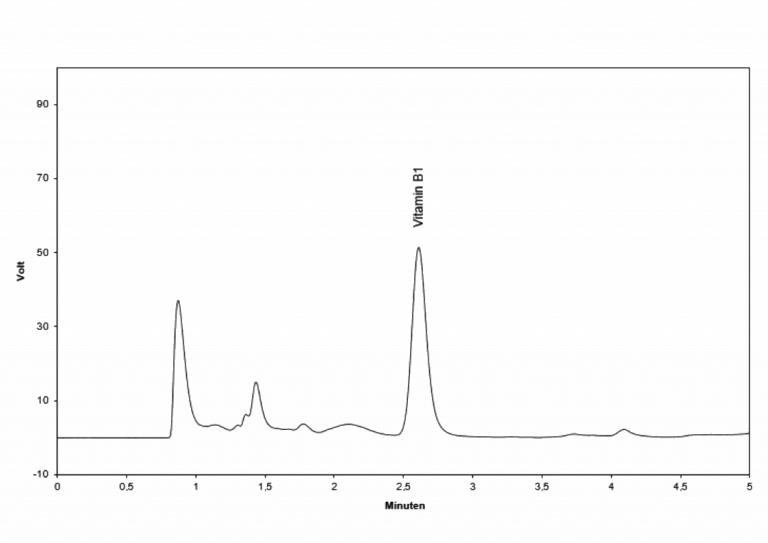
For the determination of vitamin B1 a precipitation step to remove high molecular substances is performed first. After centrifugation the supernatant is mixed with a derivatisation solution and incubated for 10 min at 60°C. The fluorescent probe is then cooled (2-8°C), centrifuged and injected into the HPLC system.
The isocratic separation via HPLC at 30°C lasts 10 minutes. The chromatograms are recorded by a fluorescence detector. The quantification is performed with the delivered EDTA-blood calibrator; the concentration is calculated via integration of the peak heights respectively areas.